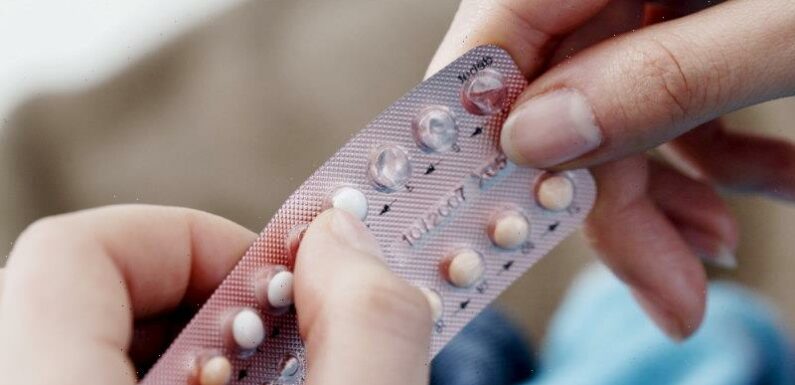
Women are being forced to pay three times as much for newer birth control pills or use older products with potentially worse side effects because the most recent contraceptive options are not subsidised.
A Senate inquiry into reproductive healthcare also heard on Tuesday that Australia was falling behind its global peers on the use of long-acting and reversible contraceptives, such as intrauterine devices.

Doctors and pharmacy groups want more products added to the Pharmaceutical Benefits Scheme.
Doctors and pharmacy groups warned that varying costs of contraception meant thousands of women were not accessing the best options for their health, as they called for more products to be added to the Pharmaceutical Benefits Scheme.
The scheme, which lists all medicines subsidised by the federal government, caps a four-month supply of the oral contraceptive pill at $30, or $7.30 for a healthcare-card holder, although some generic brands are cheaper.
But newer products that are more commonly prescribed can cost more than triple that amount: three months’ supply of the popular contraceptive pills Zoely, Yaz and Qlaira cost $87.99, $74.99 and $83.39 respectively, according to data held by reproductive non-profit MSI Health.
Women pay $76.39 for a three-month supply of progestogen-only pill Slinda, while Microlut – an older progestogen-only pill that doctors say can be less effective and cause irregular bleeding – is subsidised at $11.99 for four months.
Pharmacy Guild senior vice-president Natalie Willis said advances in technology over the past 25 years had led to new pills that offered greater benefits in terms of reduced side effects and smaller doses.
“None of these have been listed on the PBS, which is restricting access,” she said.
Pharmaceutical Society of Australia president Dr Fei Sim said affordability needed to be addressed, including for emergency contraception, also known as the morning-after pill, which was also not on the PBS and could cost up to $40 for a single dose.
“The full fee raises some concern,” she said.
“Patients from vulnerable populations should not be disadvantaged … We should not discriminate women’s access to emergency contraception based on their location, health status or financial status. That’s why we’re calling for emergency contraception to be placed on the PBS.”
Lei also called for more work to promote intrauterine devices to health professionals and consumers given lagging rates of use in Australia.
Hormonal IUDs – small devices inserted into the uterus to prevent pregnancy – are subsidised by the PBS, costing about $30, or $7.30 with a healthcare card. However, copper IUDs, which some women prefer because they do not release hormones, typically cost between $80 and $90.
Professor Danielle Mazza, an adviser on women’s health with the Royal Australian College of GPs, said IUDs reduced levels of unwanted pregnancy but there was not enough GP training or compensation to encourage their take-up.
“GPs are always telling us the rebate is too low to reflect the cost of a practice to deliver this service,” she said.
“They are essential to women’s reproductive health.”
She also called for a regulatory solution that gave Australians access to contraceptive options they needed at low or no cost. “They are essential to women’s reproductive health,” she said.
Australian Medical Association vice-president Dr Danielle McMullen agreed but said the Pharmaceutical Benefits Advisory Committee, which recommends items for the PBS, needed to receive applications from pharmaceutical companies before their products could be listed.
“[The advisory committee] can’t compel manufacturers to request listing, which has been a bit of a challenge, but we welcome more contraceptive medications on the PBS,” she said.
Asked by Greens senator Larissa Waters why important contraceptives were not subsidised, federal Health Department deputy secretary Tania Rishniw told the inquiry some companies chose not to apply to the committee.
“Without speculating … in some cases, pharmaceutical companies choose not to because they want to charge a different amount, they want to choose to set their own prices. In some cases, it might be because they don’t think the market is big enough. But the reasons will vary,” she said.
The Pharmacy Guild’s Natalie Willis suggested one potential barrier was that pharmaceutical companies applying for a listing had to prove their products were more cost-effective and effective than those that had been on the market for decades. “I think it’s a difficult process to navigate,” she said.
The inquiry also heard about uneven access to abortion services across the country, particularly for women in regional areas, ahead of a Therapeutic Goods Administration decision expected in coming months that could expand the number of health professionals who can prescribe medical abortions.
The inquiry will hand down its final report in May.
Cut through the noise of federal politics with news, views and expert analysis from Jacqueline Maley. Subscribers can sign up to our weekly Inside Politics newsletter here.
Most Viewed in Politics
From our partners
Source: Read Full Article